| Section B: The initial diagnosis, consultation with a medical oncologist |
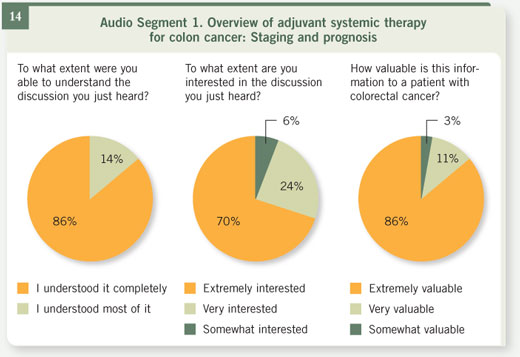
  Select excerpts from audio segment 1 Select excerpts from audio segment 1
 DR LOVE: Most patients treated with surgery for colon cancer visit a
medical oncologist postoperatively to consider chemotherapy. What are
some of the key factors in this consultation? DR LOVE: Most patients treated with surgery for colon cancer visit a
medical oncologist postoperatively to consider chemotherapy. What are
some of the key factors in this consultation? |
DR MARSHALL: When the medical oncologist meets a patient for the first
time, the most important thing we review is the pathology report. How much
cancer was there? Has it spread anywhere? What were the characteristics of the
tumor under the microscope? Then, secondly, we want to determine how well the patient tolerated surgery. Did the patient go through it with f lying colors
and recover in a week or so, or did the patient have a harder time of it?
Another important factor in making a decision about chemotherapy is the
patient’s general health status. Many patients have no other significant medical
problems, but if a patient has perhaps several other medical problems, that’s
another story. And so one takes all of those factors — the surgery, what was
found at the surgery, the characteristics of the tumor and, if you will, the
characteristics of the patient — and puts them together to make the decision
about treating the patient after surgery.
DR LOVE: Typically, these patients have had the tumor removed surgically. If
that’s the case, why would you use chemotherapy?
DR MARSHALL: These patients have had all the visible tumor removed, but,
depending on the situation, a risk exists that some seeds have been sown that
have made it past the removed lymph nodes and aren’t visible to the surgeon’s
naked eye, on CAT scans, or in blood tests. In fact, it’s unsettling, but if you
put a million cells down on a table, you can’t actually see them, because our
ability to detect such things is pretty limited.
We can define the risk for each patient, depending on the stage and the
characteristics of the tumor, assessing the chances that the patient is cured or
that the patient has these seeds. And the point of giving the chemotherapy to
these patients is to get rid of those seeds and prevent those seeds from ever
taking root and ultimately showing themselves as metastatic, or Stage IV,
disease.
DR LOVE: For patients who have surgery for localized cancer of the colon,
what are the different stages of the disease, with the different risks of developing
a future cancer relapse?
DR MARSHALL: Colon cancer has four stages. Stage I is when the tumor is
very small. It really hasn’t penetrated very deeply into the colon. And the
majority of those patients — in fact, 90 to 95 percent of them — are cured
by the surgery alone, are very unlikely to have any seeds and, therefore, don’t
receive chemotherapy.
Patients with Stage II and Stage III colon cancer have a different story. In
Stage II disease, the tumor has invaded all the way through the bowel but has
not spread to any of the lymph nodes. Treatment for this group of patients is
quite controversial. Some doctors will treat these patients with chemotherapy
and some will not. As a group, about 75 percent of Stage II patients do not
have any seeds and will not have their cancer come back and therefore are
essentially cured of their cancer after surgery. That leaves 25 percent or so that
will experience recurrence.
Patients with Stage III disease represent about a quarter to maybe a third of
all the colon cancer patients who are diagnosed in the United States. In this
group of patients, the cancer has spread to the lymph nodes, and even just one
lymph node with tumor in it qualifies the disease as Stage III. We know that the more lymph nodes that have tumor in them, the more worrying it is for
patients that they might have seeds somewhere else, such as in the liver or the
lungs. In this group, the odds are about 50-50 of having seeds or not having
seeds.
DR LOVE: For the patients who do have seeds of the tumor elsewhere, why
not just wait until they grow and cause a problem, and treat at that point?
DR MARSHALL: That’s a great question and a very common question. The real
reason is that once these seeds have taken root and have become visible metastases
or spread of the tumor, our chemotherapy drugs cannot eliminate the last
cell. Usually, our only chance at curing the cancer, at least today, is to treat
before it sets up shop, before it grows roots and is visible.
So we treat patients before we see any spread. That’s our window of opportunity
to add to the number of patients that are cured. Said another way, we, as
medical oncologists, try to kill the last cancer cells, the ones that we can’t see,
by giving chemotherapy.
DR LOVE: What about Stage IV?
DR MARSHALL: In patients with Stage IV colon cancer, the disease has already
made it past the lymph nodes and has spread to the liver or the lungs. And
traditionally, this group is not curable. Usually surgery cannot remove this
disease, which has spread. And those patients, unfortunately, do not have treatment
options that will cure them. But we do have very good treatments that
can extend their survival and help them live longer lives.
|

